1 016 295 läst ·
19 546 svar
1016k läst
19,5k svar
Coronavirus (SARS-CoV-2) nyhetstråd
Det är inte de på FHM som är tomtar, de hittar man tydligen på helt andra ställen av ditt inlägg att dömma.optimum skrev:
Nu gissar du. Corona virus klarar sig flera dagar på hårda ytor. Mer än 3 dygn enligt denna artikel.
På kartong ca 1 dygn.
[länk]
Det finns inga problem med att peta sig i ansiktet så länge händerna är rena.
Att hålla händerna rena är av största betydelse för då finns ingen risk om man oavsiktligt råkar ta sig i ansiktet vilket de flesta gör.
Det är därför jag desinficerar mitt kontor med de ytor händerna är på med spritlösning regelbundet. Och spritar händerna när jag kommer in på mitt kontor. Därför gör det inget om händerna kommer i kontakt med ansiktet.
Nu har ju FHM gått ut med att vi ska tvätta händerna och ändå skriver de att det har marginell betydelse.
Ja de är riktiga tomtar. Först gick det ut med kurser i att tvätta händerna för det var så viktigt och sedan föringar de det som inte så viktigt.
Jag föringar absolut inte som de risken att bli smittad via vad mina händer tagit i.
Fortfarande frisk. Tänk själv är bra.
Det känns som att du tillhör de som gör allt för att dö friska, vilket sannolikt inte kommer att hända…
Ja men eftersom folk här är så vetenskapliga och alltid frågar efter belägg och studier så fladdrade tanken förbi att folk kanske i allmänhet håller avstånd till någon de anser är "utklädd".P pmd skrev:

Testa de klassiska, sjuksköterska, kanin, "La Casa Papell", skelett osv, se om det blir skillnad, ännu roligare byt munskyddet mot en klassisk pestläkaredräkt?

Grekerna har hittat på ett eget dokument dessutom som man måste fylla i för att komma in. Kommer inte ihåg namnet på det, men det + covidvaccinintyg så är det ings problem. Tror det funkar med intyg om genomgången infektion och negativa tester oxå. Men vaccinintyget är ju enklast.G gaidin skrev:
En pressrelease från 1/10 om Mercks fas 3 studie av en antiviral medicin mot sars-cov-2 viruset. (Nämnt tidigare i tråden länk)
Att medicinen är från 2003 gör den inte billig. 70 dollar per dos eller 700 dollar för en 5 dagars kur får man en kur som minskar risken för sjukhusinläggning eller död med 50% vilket man tyckte var så bra att man avbryter studien och söker Emergency Use Authorization i USA.
Merck and Ridgeback’s Investigational Oral Antiviral Molnupiravir Reduced the Risk of Hospitalization or Death by Approximately 50 Percent Compared to Placebo for Patients with Mild or Moderate COVID-19 in Positive Interim Analysis of Phase 3 Study
Att medicinen är från 2003 gör den inte billig. 70 dollar per dos eller 700 dollar för en 5 dagars kur får man en kur som minskar risken för sjukhusinläggning eller död med 50% vilket man tyckte var så bra att man avbryter studien och söker Emergency Use Authorization i USA.
Merck and Ridgeback’s Investigational Oral Antiviral Molnupiravir Reduced the Risk of Hospitalization or Death by Approximately 50 Percent Compared to Placebo for Patients with Mild or Moderate COVID-19 in Positive Interim Analysis of Phase 3 Study
https://www.merck.com/news/merck-an...to-placebo-for-patients-with-mild-or-moderat/KENILWORTH, N.J. & MIAMI--(BUSINESS WIRE)-- Merck (NYSE: MRK), known as MSD outside the United States and Canada, and Ridgeback Biotherapeutics today announced that molnupiravir (MK-4482, EIDD-2801), an investigational oral antiviral medicine, significantly reduced the risk of hospitalization or death at a planned interim analysis of the Phase 3 MOVe-OUT trial in at risk, non-hospitalized adult patients with mild-to-moderate COVID-19. At the interim analysis, molnupiravir reduced the risk of hospitalization or death by approximately 50%; 7.3% of patients who received molnupiravir were either hospitalized or died through Day 29 following randomization (28/385), compared with 14.1% of placebo-treated patients (53/377); p=0.0012. Through Day 29, no deaths were reported in patients who received molnupiravir, as compared to 8 deaths in patients who received placebo. At the recommendation of an independent Data Monitoring Committee and in consultation with the U.S. Food and Drug Administration (FDA), recruitment into the study is being stopped early due to these positive results. Merck plans to submit an application for Emergency Use Authorization (EUA) to the U.S. FDA as soon as possible based on these findings and plans to submit marketing applications to other regulatory bodies worldwide.
Tror ej att denna har postats i tråden tidigare.
https://jamanetwork.com/journals/jama/fullarticle/2784015
Abstract
Importance Safety surveillance of vaccines against COVID-19 is critical to ensure safety, maintain trust, and inform policy.
Objectives To monitor 23 serious outcomes weekly, using comprehensive health records on a diverse population.
Design, Setting, and Participants This study represents an interim analysis of safety surveillance data from Vaccine Safety Datalink. The 10 162 227 vaccine-eligible members of 8 participating US health plans were monitored with administrative data updated weekly and supplemented with medical record review for selected outcomes from December 14, 2020, through June 26, 2021.
Exposures Receipt of BNT162b2 (Pfizer-BioNTech) or mRNA-1273 (Moderna) COVID-19 vaccination, with a risk interval of 21 days for individuals after vaccine dose 1 or 2 compared with an interval of 22 to 42 days for similar individuals after vaccine dose 1 or 2.
Main Outcomes and Measures Incidence of serious outcomes, including acute myocardial infarction, Bell palsy, cerebral venous sinus thrombosis, Guillain-Barré syndrome, myocarditis/pericarditis, pulmonary embolism, stroke, and thrombosis with thrombocytopenia syndrome. Incidence of events that occurred among vaccine recipients 1 to 21 days after either dose 1 or 2 of a messenger RNA (mRNA) vaccine was compared with that of vaccinated concurrent comparators who, on the same calendar day, had received their most recent dose 22 to 42 days earlier. Rate ratios (RRs) were estimated by Poisson regression, adjusted for age, sex, race and ethnicity, health plan, and calendar day. For a signal, a 1-sided P < .0048 was required to keep type I error below .05 during 2 years of weekly analyses. For 4 additional outcomes, including anaphylaxis, only descriptive analyses were conducted.
Results A total of 11 845 128 doses of mRNA vaccines (57% BNT162b2; 6 175 813 first doses and 5 669 315 second doses) were administered to 6.2 million individuals (mean age, 49 years; 54% female individuals). The incidence of events per 1 000 000 person-years during the risk vs comparison intervals for ischemic stroke was 1612 vs 1781 (RR, 0.97; 95% CI, 0.87-1.08); for appendicitis, 1179 vs 1345 (RR, 0.82; 95% CI, 0.73-0.93); and for acute myocardial infarction, 935 vs 1030 (RR, 1.02; 95% CI, 0.89-1.18). No vaccine-outcome association met the prespecified requirement for a signal. Incidence of confirmed anaphylaxis was 4.8 (95% CI, 3.2-6.9) per million doses of BNT162b2 and 5.1 (95% CI, 3.3-7.6) per million doses of mRNA-1273.
Conclusions and Relevance In interim analyses of surveillance of mRNA COVID-19 vaccines, incidence of selected serious outcomes was not significantly higher 1 to 21 days postvaccination compared with 22 to 42 days postvaccination. While CIs were wide for many outcomes, surveillance is ongoing.
https://jamanetwork.com/journals/jama/fullarticle/2784015
Abstract
Importance Safety surveillance of vaccines against COVID-19 is critical to ensure safety, maintain trust, and inform policy.
Objectives To monitor 23 serious outcomes weekly, using comprehensive health records on a diverse population.
Design, Setting, and Participants This study represents an interim analysis of safety surveillance data from Vaccine Safety Datalink. The 10 162 227 vaccine-eligible members of 8 participating US health plans were monitored with administrative data updated weekly and supplemented with medical record review for selected outcomes from December 14, 2020, through June 26, 2021.
Exposures Receipt of BNT162b2 (Pfizer-BioNTech) or mRNA-1273 (Moderna) COVID-19 vaccination, with a risk interval of 21 days for individuals after vaccine dose 1 or 2 compared with an interval of 22 to 42 days for similar individuals after vaccine dose 1 or 2.
Main Outcomes and Measures Incidence of serious outcomes, including acute myocardial infarction, Bell palsy, cerebral venous sinus thrombosis, Guillain-Barré syndrome, myocarditis/pericarditis, pulmonary embolism, stroke, and thrombosis with thrombocytopenia syndrome. Incidence of events that occurred among vaccine recipients 1 to 21 days after either dose 1 or 2 of a messenger RNA (mRNA) vaccine was compared with that of vaccinated concurrent comparators who, on the same calendar day, had received their most recent dose 22 to 42 days earlier. Rate ratios (RRs) were estimated by Poisson regression, adjusted for age, sex, race and ethnicity, health plan, and calendar day. For a signal, a 1-sided P < .0048 was required to keep type I error below .05 during 2 years of weekly analyses. For 4 additional outcomes, including anaphylaxis, only descriptive analyses were conducted.
Results A total of 11 845 128 doses of mRNA vaccines (57% BNT162b2; 6 175 813 first doses and 5 669 315 second doses) were administered to 6.2 million individuals (mean age, 49 years; 54% female individuals). The incidence of events per 1 000 000 person-years during the risk vs comparison intervals for ischemic stroke was 1612 vs 1781 (RR, 0.97; 95% CI, 0.87-1.08); for appendicitis, 1179 vs 1345 (RR, 0.82; 95% CI, 0.73-0.93); and for acute myocardial infarction, 935 vs 1030 (RR, 1.02; 95% CI, 0.89-1.18). No vaccine-outcome association met the prespecified requirement for a signal. Incidence of confirmed anaphylaxis was 4.8 (95% CI, 3.2-6.9) per million doses of BNT162b2 and 5.1 (95% CI, 3.3-7.6) per million doses of mRNA-1273.
Conclusions and Relevance In interim analyses of surveillance of mRNA COVID-19 vaccines, incidence of selected serious outcomes was not significantly higher 1 to 21 days postvaccination compared with 22 to 42 days postvaccination. While CIs were wide for many outcomes, surveillance is ongoing.
Vaccinet tappar hälften av sin effektivitet på 6 månader (risken att bli smittad) men har bibehållet skyddet (90%) mot att bli svårt sjuk för hela perioden.
Det låter ju rätt bra men funderar på man mäter skyddet mot svår sjukdom här. Om ingångsvärdet är "svårt sjuka av alla de som drabbas av Covid-19 infektion" så betyder det ju att dubbelt så många blir svårt sjuka efter 6 månader som efter 1 månad. Rimligen borde det vara så...?
""Two doses of the Pfizer/BioNTech Covid vaccine are “highly effective” at preventing hospitalisations for at least six months, a large-scale study shows, but protection against infection nearly halves over the same period.
Effectiveness against all Covid infections fell from 88% within a month of having two doses to 47% after six months, according to the research. However, effectiveness against hospitalisations remained high at 90% overall – and crucially across all variants, including delta.""
https://www.theguardian.com/world/2...against-hospitalisation-for-at-least-6-months
Det låter ju rätt bra men funderar på man mäter skyddet mot svår sjukdom här. Om ingångsvärdet är "svårt sjuka av alla de som drabbas av Covid-19 infektion" så betyder det ju att dubbelt så många blir svårt sjuka efter 6 månader som efter 1 månad. Rimligen borde det vara så...?
""Two doses of the Pfizer/BioNTech Covid vaccine are “highly effective” at preventing hospitalisations for at least six months, a large-scale study shows, but protection against infection nearly halves over the same period.
Effectiveness against all Covid infections fell from 88% within a month of having two doses to 47% after six months, according to the research. However, effectiveness against hospitalisations remained high at 90% overall – and crucially across all variants, including delta.""
https://www.theguardian.com/world/2...against-hospitalisation-for-at-least-6-months

Om du vill tränga in i det så bör detta vara den studie de avser: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)02183-8/fulltextUlltand skrev:
Två studier som handlar om effekten av en tredje vaccinationsdos.
https://www.nejm.org/doi/full/10.1056/NEJMoa2114255
Abstract
BACKGROUND
On July 30, 2021, the administration of a third (booster) dose of the BNT162b2 messenger RNA vaccine (Pfizer–BioNTech) was approved in Israel for persons who were 60 years of age or older and who had received a second dose of vaccine at least 5 months earlier. Data are needed regarding the effect of the booster dose on the rate of confirmed coronavirus 2019 disease (Covid-19) and the rate of severe illness.
METHODS
We extracted data for the period from July 30 through August 31, 2021, from the Israeli Ministry of Health database regarding 1,137,804 persons who were 60 years of age or older and had been fully vaccinated (i.e., had received two doses of BNT162b2) at least 5 months earlier. In the primary analysis, we compared the rate of confirmed Covid-19 and the rate of severe illness between those who had received a booster injection at least 12 days earlier (booster group) and those who had not received a booster injection (nonbooster group). In a secondary analysis, we evaluated the rate of infection 4 to 6 days after the booster dose as compared with the rate at least 12 days after the booster. In all the analyses, we used Poisson regression after adjusting for possible confounding factors.
RESULTS
At least 12 days after the booster dose, the rate of confirmed infection was lower in the booster group than in the nonbooster group by a factor of 11.3 (95% confidence interval [CI], 10.4 to 12.3); the rate of severe illness was lower by a factor of 19.5 (95% CI, 12.9 to 29.5). In a secondary analysis, the rate of confirmed infection at least 12 days after vaccination was lower than the rate after 4 to 6 days by a factor of 5.4 (95% CI, 4.8 to 6.1).
CONCLUSIONS
In this study involving participants who were 60 years of age or older and had received two doses of the BNT162b2 vaccine at least 5 months earlier, we found that the rates of confirmed Covid-19 and severe illness were substantially lower among those who received a booster (third) dose of the BNT162b2 vaccine.
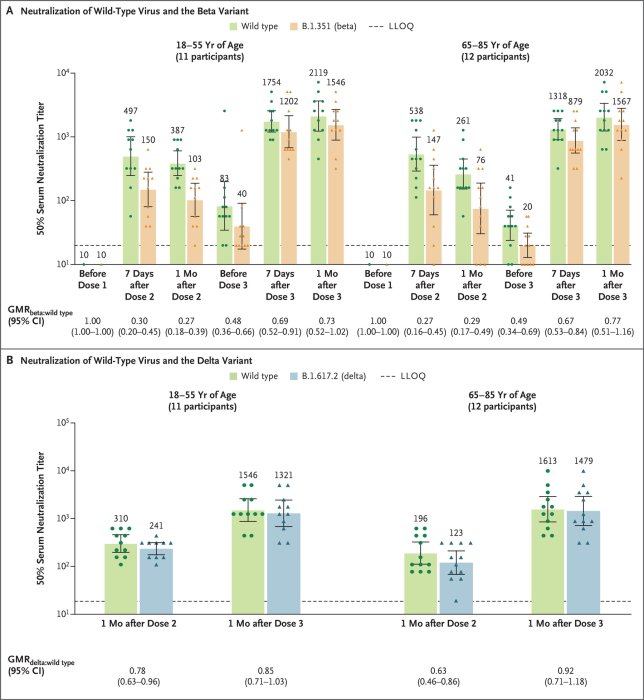
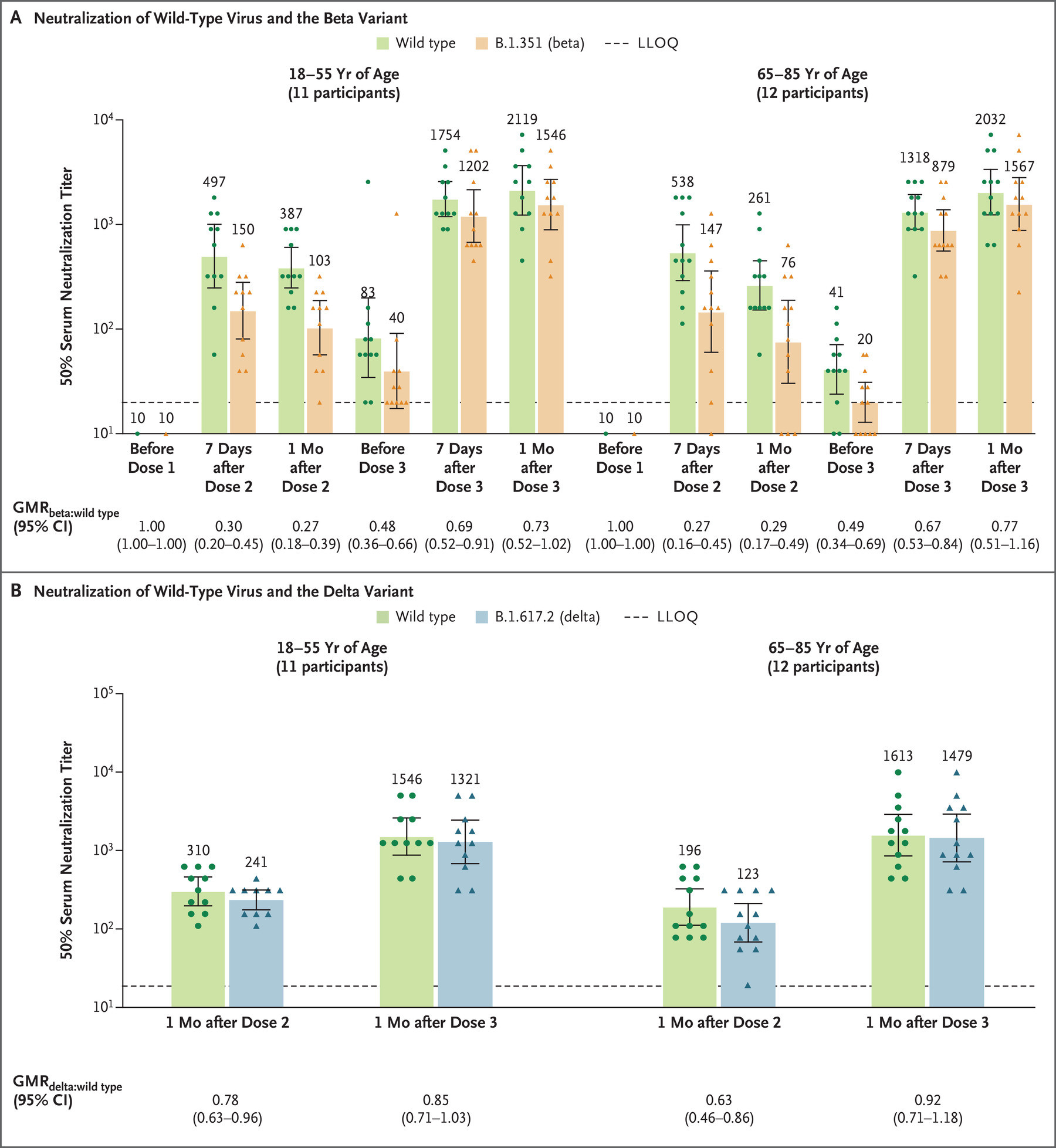
https://www.nejm.org/doi/full/10.1056/NEJMc2113468
En mindre studie där man mätt serums virusneutraliserande effekt efter vaccinationsbooster.
https://www.nejm.org/doi/full/10.1056/NEJMoa2114255
Abstract
BACKGROUND
On July 30, 2021, the administration of a third (booster) dose of the BNT162b2 messenger RNA vaccine (Pfizer–BioNTech) was approved in Israel for persons who were 60 years of age or older and who had received a second dose of vaccine at least 5 months earlier. Data are needed regarding the effect of the booster dose on the rate of confirmed coronavirus 2019 disease (Covid-19) and the rate of severe illness.
METHODS
We extracted data for the period from July 30 through August 31, 2021, from the Israeli Ministry of Health database regarding 1,137,804 persons who were 60 years of age or older and had been fully vaccinated (i.e., had received two doses of BNT162b2) at least 5 months earlier. In the primary analysis, we compared the rate of confirmed Covid-19 and the rate of severe illness between those who had received a booster injection at least 12 days earlier (booster group) and those who had not received a booster injection (nonbooster group). In a secondary analysis, we evaluated the rate of infection 4 to 6 days after the booster dose as compared with the rate at least 12 days after the booster. In all the analyses, we used Poisson regression after adjusting for possible confounding factors.
RESULTS
At least 12 days after the booster dose, the rate of confirmed infection was lower in the booster group than in the nonbooster group by a factor of 11.3 (95% confidence interval [CI], 10.4 to 12.3); the rate of severe illness was lower by a factor of 19.5 (95% CI, 12.9 to 29.5). In a secondary analysis, the rate of confirmed infection at least 12 days after vaccination was lower than the rate after 4 to 6 days by a factor of 5.4 (95% CI, 4.8 to 6.1).
CONCLUSIONS
In this study involving participants who were 60 years of age or older and had received two doses of the BNT162b2 vaccine at least 5 months earlier, we found that the rates of confirmed Covid-19 and severe illness were substantially lower among those who received a booster (third) dose of the BNT162b2 vaccine.
https://www.nejm.org/doi/full/10.1056/NEJMc2113468
En mindre studie där man mätt serums virusneutraliserande effekt efter vaccinationsbooster.
Inloggade ser högupplösta bilder
Logga in
Skapa konto
Gratis och tar endast 30 sekunder

Går den medicinen att använda som profylax?blackarrow skrev:
En pressrelease från 1/10 om Mercks fas 3 studie av en antiviral medicin mot sars-cov-2 viruset. (Nämnt tidigare i tråden länk)
Att medicinen är från 2003 gör den inte billig. 70 dollar per dos eller 700 dollar för en 5 dagars kur får man en kur som minskar risken för sjukhusinläggning eller död med 50% vilket man tyckte var så bra att man avbryter studien och söker Emergency Use Authorization i USA.
Merck and Ridgeback’s Investigational Oral Antiviral Molnupiravir Reduced the Risk of Hospitalization or Death by Approximately 50 Percent Compared to Placebo for Patients with Mild or Moderate COVID-19 in Positive Interim Analysis of Phase 3 Study
[länk]
Jag är kanske inte helt alert så här dags, men min invändning är att om skyddet mot att bli svårt sjuk bibehålls till 90 % efter sex månader så kan knappast dubbelt så många bli svårt sjuka efter sex månader jämfört med efter en månad.Vaccinet tappar hälften av sin effektivitet på 6 månader (risken att bli smittad) men har bibehållet skyddet (90%) mot att bli svårt sjuk för hela perioden.
Det låter ju rätt bra men funderar på man mäter skyddet mot svår sjukdom här. Om ingångsvärdet är "svårt sjuka av alla de som drabbas av Covid-19 infektion" så betyder det ju att dubbelt så många blir svårt sjuka efter 6 månader som efter 1 månad. Rimligen borde det vara så...?
""Two doses of the Pfizer/BioNTech Covid vaccine are “highly effective” at preventing hospitalisations for at least six months, a large-scale study shows, but protection against infection nearly halves over the same period.
Effectiveness against all Covid infections fell from 88% within a month of having two doses to 47% after six months, according to the research. However, effectiveness against hospitalisations remained high at 90% overall – and crucially across all variants, including delta.""
[länk]